Over the following decades DES was marketed and prescribed for a bewildering and often contradictory range of conditions: to slow and prevent aging; to stop hot flushes and as treatment for other menopausal symptoms; to prevent miscarriage, for pregnancy maintenance, as a pregnancy “tonic”; as the oral contraceptive pill; as the ‘morning after’ contraceptive pill; to stunt the growth of tall girls; to suppress lactation; as a hormonal pregnancy test; to treat acne…
During pregnancy
Shortly after it was synthesised, DES was being touted as a treatment for late-pregnancy complications and for high risk pregnancies, such as women with diabetes. Let’s be very clear here: this was not based on any scientific research and DES did not prevent miscarriage. In fact it increased the risk of miscarriage and foetal death, and was subsequently used as the “morning-after” contraceptive pill.
Sir E. Charles Dodds, the co-developer of stilboestrol, was against the drug being given to healthy women, and he was particularly aghast when told it was being used to “prevent miscarriage”. He had published research in 1938 showing the drug actually prevented or ended pregnancies in rabbits and rats.
The Smiths of Boston
Dr George van Sichlen Smith (Head of the Ob/Gyn Department at Harvard Medical School, 1942-1967) and his wife Dr Olive Watkins Smith (a biochemist) theorised that the new drug would be of value in the treatment of impending miscarriage and late pregnancy complications. This was based on the earlier discovery that progesterone levels dropped prior to complications in pregnancy. They hypothesised that the administration of DES would be of therapeutic value because it was thought to upset and bypass the balancing effect of the pituitary gland and stimulate the body’s own production of progesterone.
“It was found, however, that diethylstilbestrol, unlike naturally occurring estrogens, was not depressed in its pituitary stimulating effects by the presence of progesterone and might theoretically, therefore, provide an ideal agent for preventing progesterone deficiency in pregnancy.” Smith and Smith (1941)
However they were soon promoting DES as a treatment to prevent miscarriage. That is, to be given prophylactically to women with a history of prior miscarriage or pregnancy complications. They published papers that detailed the “Smith regimen”, giving instructions on exact dosages of DES to be given. They encouraged any interested doctor reading the article to try out their new “wonder drug”. Pharmaceutical companies assisted the research, offering free trials of DES to interested physicians.
“The present study, a clinical evaluation of our concept concerning the action of diethylstilbestrol in human pregnancy, was started in the fall of 1943 and is still in progress…The writer would like to emphasize that the credit for the present contribution belongs to the 117 obstetricians who not only followed our recommendations but were willing to pool their results and send us a complete record of each treated case.”
OW Smith (1948)
Of course we don’t know how many other doctors, in the US and internationally, simply followed the directions given and prescribed the new wonder drug to their pregnant patients.
In 1949 there was a considerable shift, with DES suddenly being recommended as beneficial for any pregnancy. The Smiths presented THE INFLUENCE OF DIETHYLSTILBESTROL ON THE PROGRESS AND OUTCOME OF PREGNANCY AS BASED ON A COMPARISON OF TREATED AND UNTREATED PRIMIGRAVIDAS at the Annual Conference of the American Gynaecology Society of 1949.
In an attempt to be ‘scientific’ and they wanted the two study groups as homogenous as possible, so only first time mothers expecting a normal pregnancy were allowed in the ‘DES treatment’ and ‘untreated’ groups. Any high risk pregnancy (the very condition DES supposedly treated) was excluded from the study. This selection of ‘normal’ primigravidas as subjects was to have to affect the subsequent clinical use of DES. The subjective comments made by the authors, such as DES babies were healthier and stronger and that DES appeared to render normal gestations ‘more normal’, had far-reaching ramifications on how DES was prescribed.
There were criticisms of the methodology, particularly the fact there was no control group only an untreated comparison group. The controversy itself led to many more "experiments" being conducted on unsuspecting women attending hospital ante-natal clinics, not only in the United States but other countries including Britain and Australia.
The Dieckmann Study 1953
The largest of these subsequent studies DOES THE ADMINISTRATION OF DIETHYSTILBESTROL DURING PREGNANCY HAVE THERAPEUTIC VALUE? was conducted by Dr William DIeckmann and colleagues of the University of Chicago. This study is one of the first large-scale, prospective double-blind, randomised clinical trials (RCT) reported in medical literature, and involved 2,000 women attending the Chicago Lying-In Maternity Hospital. The findings of this study showed, to the surprise of the researchers, that the DES-treated group experienced higher rates of miscarriage, premature labour and neonatal death than the control group. The authors concluded that DES was no more effective at preventing miscarriage than bed rest. While they noted that the miscarriage rate was higher in the DES treated group than the control group, they concluded that “the total number of patients was too small to be statistically significant.”
A reanalysis of the data using modern statistical methods found that, although the women receiving DES were 1.8 times more likely to miscarry than the control group, this was not statistically significant simply because the overall sample size was too small. The number of subjects had been arbitrarily picked and, based on current statistical knowledge and criteria, it is now known a much larger sample size was required to handle the number of study variables and subset analyses.
DES as a pregnancy tonic
Despite the finding that DES did not prevent miscarriage, clinically the Dieckmann study was not influential as DES was already entrenched as standard obstetric clinical practice. The Smiths’ reaction to the Dieckmann study was to simply restate their conviction that DES reduced complications of pregnancy and had “saved many babies”. In a 1954 article they reaffirmed their belief that DES would even “make a normal pregnancy more normal” and recommended commencement of DES therapy as a prophylactic measure as soon as pregnancy was confirmed.
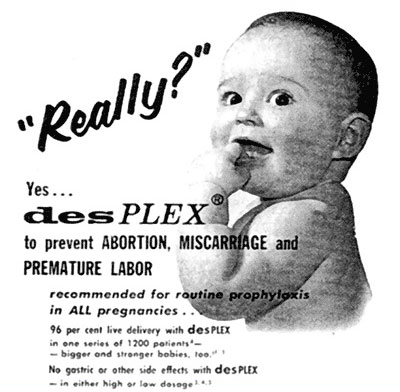
DES was being marketed as a ‘pregnancy tonic’, mixed with vitamins and recommended for all pregnancies. This 1957 advertisement for DesPLEX shows DES is now mixed with vitamins and minerals, and “recommended for routine prophylaxis in ALL pregnancies.”
In fact, many DES mothers believed they were taking vitamins.
DES was often imported, repackaged and re-branded. For example Diesavite, a very popular Australian brand that combined stilboestrol with vitamins and supplements, appears to be Australia’s version of DesPLEX. It contained a range of vitamins and minerals and, oh yes, 25 mg of stilboestrol.
So effective was the marketing to doctors of this ‘pregnancy tonic’ that many doctors didn’t realise that the drug contained stilboestrol and thought they were prescribing only vitamins.